
Trigeminal Neuralgia
What You Need to Know
- Trigeminal neuralgia most frequently affects people older than 50, and the condition is more common in women than men.
- Trigeminal neuralgia is the most common cause of facial pain and is diagnosed in approximately 15,000 people per year in the United States.
- Trigeminal neuralgia pain is exceptionally severe. Although the condition is not life-threatening, the intensity of the pain can be debilitating.
- Trigeminal neuralgia relief is possible: Medical and surgical treatments can bring the pain under control, especially when managed by an expert physician and surgeon.
What is trigeminal neuralgia?
Trigeminal neuralgia is a condition characterized by pain coming from the trigeminal nerve, which starts near the top of the ear and splits in three, toward the eye, cheek and jaw. We have two trigeminal nerves: one for each side of our face, but trigeminal neuralgia pain most commonly affects only one side.
The pain of trigeminal neuralgia is unlike facial pain caused by other problems. It is often described as stabbing, lancinating or electrical in sensation and so severe that the affected person cannot eat or drink. The pain travels through the face in a matter of seconds, but as the condition progresses, the pain can last minutes and even longer.
Trigeminal neuralgia is sometimes known as tic douloureux, which means "painful tic."
Causes of Trigeminal Neuralgia
Trigeminal neuralgia usually occurs spontaneously, but is sometimes associated with facial trauma or dental procedures.
The condition may be caused by a blood vessel pressing against the trigeminal nerve, also known as vascular compression. Over time, the pulse of an artery rubbing against the nerve can wear away the insulation, which is called myelin, leaving the nerve exposed and highly sensitive.
The resulting symptoms can be similar to those caused by dental problems, and sometimes people with undiagnosed trigeminal neuralgia explore multiple dental procedures in an effort to control the pain.
Multiple sclerosis or a tumor — while rare — can also cause trigeminal neuralgia. Researchers are exploring whether or not postherpetic neuralgia (caused by shingles) can be related to this condition.
Trigeminal Neuralgia Symptoms
Trigeminal neuralgia occurs more often in women than men, is more common in older people (usually 50 and older), and occurs more on the right than the left. It doesn’t usually run in families.
Trigeminal neuralgia symptoms may include:
- Episodes of sharp, intense, stabbing pain in the cheek or jaw that may feel like an electric shock. Pain episodes may be triggered by anything touching the face or teeth, including shaving, applying makeup, brushing teeth, touching a tooth or a lip with the tongue, eating, drinking or talking — or even a light breeze or water hitting the face.
- Periods of relief between episodes.
- Anxiety from the thought of the pain returning.
Trigeminal Neuralgia Pain
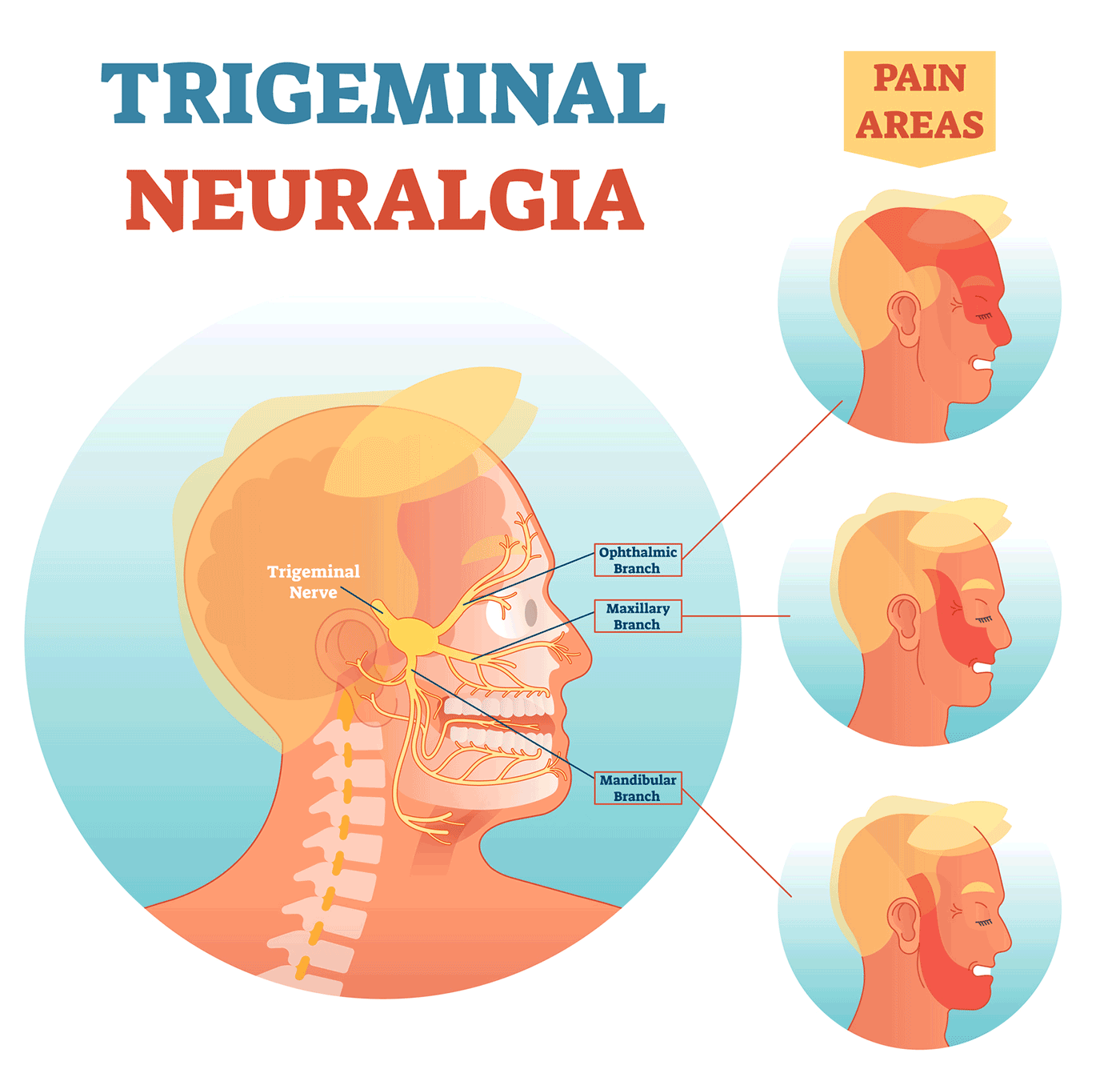
The trigeminal nerve splits off into three branches: ophthalmic, maxillary and mandibular. Each branch provides sensation to different areas of the face. Depending on which branch and which part of the nerve is irritated, trigeminal neuralgia pain can be felt anywhere in the face. Most commonly, it is felt in the lower part of the face. The intensity of the pain is exceptional: Some people report it to be more severe than experiencing a heart attack, passing a kidney stone or even giving birth.
A flare-up of trigeminal neuralgia may begin with tingling or numbness in the face. Pain occurs in intermittent bursts that last anywhere from a few seconds to two minutes, becoming more and more frequent until the pain is almost continuous.
Flare-ups may continue for a few weeks or months followed by a pain-free period that can last a year or more. Although trigeminal neuralgia pain may seem to disappear, it always comes back, often with more intensity.
In some cases, instead of sharp, stabbing pain, trigeminal neuralgia appears as a persisting dull ache. This and other symptom variations are sometimes described as “atypical trigeminal neuralgia.”
Trigeminal Neuralgia Diagnosis
Diagnosing trigeminal neuralgia involves a physical exam and a detailed medical history to rule out other causes of facial pain. Your health care provider (usually your primary care doctor or a neurologist) will ask about the frequency and intensity of the pain, what seems to set it off and what makes it feel better or worse. Since there is no single test for trigeminal neuralgia, getting to the nature of the pain is key to the diagnosis.
Your provider may also recommend imaging or laboratory tests, such as a CAT scan or a high-resolution MRI of the trigeminal nerve and surrounding areas. These tests can help determine if the pain is caused by a tumor or blood vessel abnormality, or by undiagnosed multiple sclerosis. Certain advanced MRI techniques may help the doctor see where a blood vessel is pressing against a branch of the trigeminal nerve.
Trigeminal Neuralgia Treatment
Most common over-the-counter and prescription pain medicines don't work for people with trigeminal neuralgia, but many modern treatments can reduce or eliminate the pain. The doctor may recommend one or more of these approaches:
Trigeminal Neuralgia Medications
Many people who suffer from trigeminal neuralgia successfully manage this condition for many years with medication. Trigeminal neuralgia drug therapy uses some of the same medicines prescribed for controlling seizures, which includes carbamazepine, gabapentin and similar agents. Regular blood tests may be required for some medications to check your white blood cell count, platelets, sodium levels and liver function.
Your neurologist or primary care physician can help you select the best drug and the most appropriate dosage. Most patients start out on low doses, gradually increasing the dose under clinical supervision until they achieve the best pain relief with the least amount of side effects.
Trigeminal Nerve Blocks
Nerve blocks are injections (with a steroid medication or another agent) made at various parts of the nerve to reduce pain. They may provide temporary pain relief for people with trigeminal neuralgia. Multiple injections are usually needed to achieve the desired relief, and the effects may have different durations for different people.
Surgery for Trigeminal Neuralgia
If medication no longer controls your trigeminal neuralgia pain despite the increased dosage, or if the side effects are intolerable, there are several surgical procedures to consider. It helps to learn about these options before you are in urgent need of relief so you and your doctor have time to evaluate them. Your overall health, age, pain level and the availability of the procedure will all factor in to this decision. Most people with trigeminal neuralgia are candidates for any of the surgical treatment options — your doctor can help you decide which ones and in what order you should consider them.
The surgery for trigeminal neuralgia is delicate and precise since the involved area is very small. Look for experienced neurosurgeons who see and treat a large number of people with trigeminal neuralgia.
Rhizotomy
There are several kinds of rhizotomies for trigeminal neuralgia, which are all outpatient procedures performed under general anesthesia in the operating room. The surgeon inserts a long needle through the cheek on the affected side of the face and uses an electrical current (heat) or a chemical (glycerin or glycerol) to deaden the pain fibers of the trigeminal nerve. For those undergoing trigeminal neuralgia rhizotomy for the first time, the chemical approach is typically recommended. Those who have the procedure repeated often benefit from both the chemical and the heat treatment delivered in the same session.
The procedure takes about 30 minutes and most patients go home several hours later with less to no pain. Out of the three surgical options, rhizotomy offers the most immediate relief from trigeminal neuralgia pain. You may experience some swelling or bruising of the cheek. Your doctor will prescribe pain medications and, if necessary, give you a plan to gradually discontinue your medications.
Rhizotomy provides pain relief to about 80% of patients with trigeminal neuralgia, but it’s a temporary solution that usually lasts one to three years, until the nerve regrows.
Rhizotomy is a recommended surgical treatment for patients with trigeminal neuralgia resulting from multiple sclerosis (MS). It is minimally invasive and can be safely repeated, since the pain is more likely to come back due to the progression of MS.
Microvascular Decompression (MVD) Surgery
Microvascular decompression (MVD) surgery is regarded as the most long-lasting treatment for trigeminal neuralgia caused by blood vessel compression, and it helps about 80% of people with this diagnosis. It is suitable for people in good health who can tolerate surgery and general anesthesia, and whose lifestyles can accommodate a recovery period of four to six weeks.
The goal of the MVD surgery is to separate the blood vessel from the trigeminal nerve by placing a cushion made of Teflon between them. The surgeon makes an incision behind the ear and removes a small piece of the skull to gain access to the trigeminal nerve and surrounding blood vessels. Then, the surgeon places a cushion around the blood vessel so it no longer compresses or rubs against the nerve. The surgery takes two to three hours, and patients can expect to spend up to a couple of days in the hospital for recovery and observation. The pain relief with MVD is quick but not immediate.
The risks of this surgery include cerebral spinal fluid leak, hearing loss (if the hearing nerve is affected) and facial numbness that may persist in some cases. In rare cases, bleeding, infection, seizures and paralysis are possible.
In some people treated with MVD surgeries, trigeminal neuralgia pain may return, possibly due to the blood vessels growing back. If this happens, your doctor will help you choose other options. The MVD procedure is rarely repeated.
Stereotactic Radiosurgery
Stereotactic radiosurgery, sometimes known as CyberKnife or Gamma Knife treatment, is another outpatient procedure that can be used to treat trigeminal neuralgia. It involves a very concentrated and precise beam of radiation that is directed at the trigeminal nerve to relieve the pain. The surgeons use MRI and CT scans to generate a detailed image of the head to locate the trigeminal nerve. Then, they work with radiation oncologists and physicists to deliver the radiation treatment, which takes about 45 minutes.
This procedure is painless and is performed without anesthesia. Close to 70% of patients experience significant pain relief within weeks of undergoing stereotactic radiosurgery for trigeminal neuralgia. The relief may last for several years, but in some cases the nerve may recover from radiation and resume transmitting pain.
Side effects are minimal and may include fatigue and facial numbness, so the recovery time is brief. Because this procedure involves high doses of radiation delivered near the brain, it’s recommended that patients receive it no more than two times as a treatment for trigeminal neuralgia.
Trigeminal Neuralgia Surgery | Michelle's Story
Clinical Trials
Patients who have tried medications and surgical options and keep experiencing debilitating pain may qualify for clinical trials to help manage trigeminal neuralgia. These studies typically explore new medications that have a potential to provide the desired pain relief.
Speak to your neurosurgeon if you are interested in joining a clinical trial for trigeminal neuralgia.
Acupuncture and Other Integrative Medicine Treatments
Acupuncture involves insertion of thin needles along the “trigger points” to provide pain relief. Some people with trigeminal neuralgia report that acupuncture helps reduce intensity and/or frequency of flare-ups.
Meditation, wellness clinics and lifestyle modification programs are also options for those looking for more natural trigeminal neuralgia treatments or a supplemental treatment after surgery.
Caring for a Loved One with Trigeminal Neuralgia
Although not fatal, trigeminal neuralgia pain and the anxiety it causes can erode the quality of life not only for the person suffering, but for those around them. Understanding the severity of the pain the person is going through and being accommodating are the first steps to caring for a loved one with trigeminal neuralgia. Other steps may include:
- Helping your loved one stay on track with his or her medications and communicating about the success of the treatment.
- Encouraging doctor visits and exploring other treatment options when medications stop working.
- Helping locate and coordinate appointments with doctors who can offer evaluations and second opinions.
It is essential to work closely with experienced and compassionate health care providers who can help find the best therapeutic approach for each person.
